Shop & Wellness In India
Experience the highest quality CBD oil, crafted for balance, calm, and well-being. Explore our curated range of CBD products at India’s leading CBD online store. Find your perfect blend for a healthier, happier lifestyle!

Delicious CBD Gummies for Wellness Anytime, Anywhere
Enhance your wellness with delicious, easy-to-take CBD gummies—perfect for balance and relaxation anytime, anywhere!

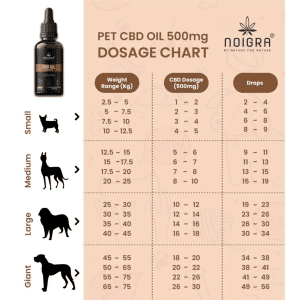
CBD Oil for Pets – Boost Your Pet's Well-Being
Give your pet the care they deserve with all-natural CBD oil. Trusted brands like Polyherbs, BOHECO, Neet CBD, Ananta Hemp, Cannavedic, Cannazo India, and more offer safe, effective formulas to enhance relaxation and overall wellness for your furry companion.

Sleep Peacefully with CBD Oil
Experience the natural way to promote relaxation and sleep. Say goodbye to sleepless nights and hello to peaceful, restorative rest. Try our premium CBD oil today and wake up feeling refreshed!"

Shop & Wellness In India
India’s most trusted CBD brands are now available in one place, including Polyherbs, BOHECO, Neet CBD, Ananta Hemp, Cannavedic, Cannazo India, and more.
Delicious CBD Gummies for Wellness Anytime, Anywhere
Enhance your wellness with delicious, easy-to-take CBD gummies—perfect for balance and relaxation anytime, anywhere!
CBD Oil for Pets – Boost Your Pet's Well-Being
Give your pet the care they deserve with all-natural CBD oil. Trusted brands like Polyherbs, BOHECO, Neet CBD, Ananta Hemp, Cannavedic, Cannazo India, and more offer safe, effective formulas to enhance relaxation and overall wellness for your furry companion.
Sleep Peacefully with CBD Oil
Experience the natural way to promote relaxation and sleep. Say goodbye to sleepless nights and hello to peaceful, restorative rest. Try our premium CBD oil today and wake up feeling refreshed!"
-


-


-


-

 ₹1,750 – ₹3,999Select options This product has multiple variants. The options may be chosen on the product page
₹1,750 – ₹3,999Select options This product has multiple variants. The options may be chosen on the product page -
 ₹4,000Select options This product has multiple variants. The options may be chosen on the product page
₹4,000Select options This product has multiple variants. The options may be chosen on the product page -
 ₹3,800 – ₹9,200Select options This product has multiple variants. The options may be chosen on the product page
₹3,800 – ₹9,200Select options This product has multiple variants. The options may be chosen on the product page -
₹3,999 – ₹8,999Select options This product has multiple variants. The options may be chosen on the product page
-
₹1,299 – ₹3,499Select options This product has multiple variants. The options may be chosen on the product page
-
-
-
₹2,499 – ₹5,499Select options This product has multiple variants. The options may be chosen on the product page
-
-
₹7,038 – ₹12,999Select options This product has multiple variants. The options may be chosen on the product page
-
-
₹2,500 – ₹4,000Select options This product has multiple variants. The options may be chosen on the product page




















-
-
₹1,000 – ₹1,500Select options This product has multiple variants. The options may be chosen on the product page
-
₹4,900 – ₹9,500Select options This product has multiple variants. The options may be chosen on the product page
-
-
-
-
₹7,999 – ₹19,999Select options This product has multiple variants. The options may be chosen on the product page















-
-
-
-
₹5,500 – ₹10,000Select options This product has multiple variants. The options may be chosen on the product page
-
₹1,999 – ₹3,599Select options This product has multiple variants. The options may be chosen on the product page
-
₹15,999 – ₹27,999Select options This product has multiple variants. The options may be chosen on the product page
-
-
-
-













-
-
-
₹3,800Select options This product has multiple variants. The options may be chosen on the product page
-
-
-
₹1,999 – ₹5,999Select options This product has multiple variants. The options may be chosen on the product page
-
-
₹1,999 – ₹5,999Select options This product has multiple variants. The options may be chosen on the product page
-

















-
₹499 – ₹1,599Select options This product has multiple variants. The options may be chosen on the product page
-
₹399 – ₹1,499Select options This product has multiple variants. The options may be chosen on the product page
-
₹299 – ₹699Get notified This product has multiple variants. The options may be chosen on the product page
-
₹849 – ₹2,799Select options This product has multiple variants. The options may be chosen on the product page
-
-
-
₹849 – ₹1,249Select options This product has multiple variants. The options may be chosen on the product page
-
₹899 – ₹1,750Select options This product has multiple variants. The options may be chosen on the product page
-
-
₹849 – ₹1,299Select options This product has multiple variants. The options may be chosen on the product page


































Aarogya CBD
4.8
 56 Reviews
56 Reviews

AROGYA CBD oil
Timely delivery. Bottle had leaked a little, so packaging could be better. Trying it for the first time for chronic neuropathic pain from operated degenerative disc disease and spondylolisthesis. Have used 0.5 ml every evening for past 10 odd days. Not felt any miraculous pain relief, but definitely, use of other SOS pain medication has reduced. Need to watch for a bit longer. One big change is a willingness to go for a walk and exercise a little. That is progress. Even if I could drop a few kilos weight, I will be more comfortable. No major side effects except for a little dryness of the mouth and consequent incease in water intake. I still have disturbed sleep, but am able to go back to sleep quickly. Feel positive. I hope this helps others.
I had a consultation call with Dr
I had a consultation call with Dr. Shaikh. He is a very knowledgeable person in the field of cannabis Medicine and he went to the depth of my issues to recommend me the best CBD oil.. Thank you so much to Dr Shaikh and entire team.. I am ordering my oil now and will post the feedback of that as well after a month hopefully
Everything was TOP NOTCH
Everything was TOP NOTCH, starting from customer support help, shipping time, and delivered product quality. CBD oil really helped my mom with her lower back and knee pain which even APOLLO doctors(tried 3 Neurologists) could not fix. All thanks to experience CBD Doctors available in Aarogya CBD platform and best adviced CBD medicine. Thanks Again Aarogya CBD